It begins with a heart-sinking moment of disorientation. Perhaps your mother can’t recall a conversation you had just an hour ago, or your husband, usually so capable, finds himself lost in the aisles of the grocery store he has visited for thirty years.
As a caregiver, your mind doesn't just wander toward concern; it often leaps straight to the word “dementia.”

Before you allow that fear to take root, it is essential to understand that these moments of “brain fog” require objective investigation, not just anxious observation. Cognitive screening tests are the vital first step in moving from paralyzing worry to empowered action.
While names like the Montreal Cognitive Assessment (MoCA) or the Mini-Mental Status Exam (MMSE) may sound intimidatingly clinical, they are simply tools designed to help, not to define. They are the compass that helps you navigate the uncertainty of aging, turning a vague sense of dread into a structured medical conversation.
The “Gold Standard” in Dementia Screening is Shifting: Why Sensitivity Matters
For decades, the Mini-Mental Status Exam (MMSE) was the cornerstone of cognitive testing. However, modern clinical practice has shifted decisively toward the Montreal Cognitive Assessment (MoCA).
The reason is a stark difference in sensitivity: research indicates that the MMSE catches only about 18% of Mild Cognitive Impairment (MCI) cases, whereas the MoCA boasts a 90% to 100% sensitivity rate for detecting these early, subtle shifts.
This preferential shift to the MoCA matters because of a domain known as “Executive Function.” This involves the brain’s “command center” responsibilities: planning, organization, and mental flexibility.
While the MMSE focuses heavily on memory and orientation, the MoCA tests nine key cognitive domains, including Abstraction (asking how a train and a bicycle are alike), Naming (identifying animals like a rhinoceros or a camel), and Attention (tapping one's hand when hearing a specific letter).
Pro Tip: Relying on a less sensitive test, such as the MMSE, can lead to a dangerous “false sense of security.” If an older adult passes an outdated screen while their executive function is actually beginning to fray, the family may miss the critical window where lifestyle changes and early interventions are most effective. A “miss” in the early stages isn't just a clerical error; it’s lost time that can never be recovered.
The “Imposter Factor”: Low Scores Aren't Always Dementia
A crucial realization for any caregiver is that these screens are exactly that – screens, not final diagnoses. They are designed to trigger further investigation, not to provide a life sentence.
A low score on a test like the MoCA or even the Abbreviated Mental Test Score (AMTS), where a score of 6 or lower indicates impairment, does not automatically equal an Alzheimer’s Disease diagnosis.
Several treatable “imposter” conditions can cause a patient to perform poorly on a cognitive screen, including:
- Urinary Tract Infections (UTIs)
- Vitamin B12 deficiency
- Sleep apnea
- Severe depression or anxiety
- Thyroid issues
If a cognitive screening result indicates impairment, the next step is to request a full medical panel, including blood tests and neuroimaging such as an MRI, to rule out reversible causes.
Empowerment at the Kitchen Table: The SAGE Test
For families who want to be proactive before their next doctor’s visit, the Self-Administered Gerocognitive Exam (SAGE) is a breakthrough for at-home health management. Developed by researchers at The Ohio State University, this 15-minute pen-and-paper test allows an older adult to assess their own cognitive health in a comfortable environment.
The SAGE test is uniquely designed to be robust. It offers four versions to prevent the “practice effect,” in which a person might score higher simply because they remember the questions from the previous year.
The SAGE test for dementia also includes an “Education Adjustment,” which adds 1 point to the total score for those with 12 years or fewer of formal education, ensuring fair results regardless of background.
Specific tasks on the SAGE test include:
- Calculating change: Figuring out how much change you’d receive back from a $20 bill after buying $13.45 in groceries.
- Fluency: Writing down the names of 12 different animals or pets.
- Precision Drawing: Completing a clock face where the hands are specifically labeled “L” for the long hand and “S” for the short hand.
Pro Tip: The SAGE test shifts the power dynamic back to the family. Often, caregivers encounter a “wait and see” attitude from busy physicians. By walking into an appointment with a completed SAGE test in hand, you provide the doctor with an objective, data-driven starting point that is difficult to dismiss. You move from being an observer of decline to an advocate for care.
More Than Telling Time: The Secret Language of the Clock
The “Clock Drawing Test” is a recurring element in the Mini-Cog, the MoCA, and the SAGE for a reason. It is deceptively complex. The patient is asked to draw a large clock face, place all the numbers, and set the hands to a specific time – usually “10 minutes after 11.”
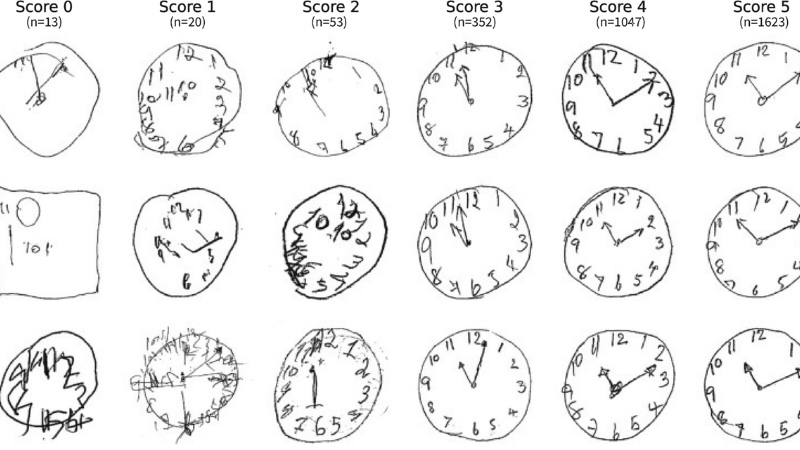
The Clock Drawing Test task is a window into the brain's visuospatial and executive health. It requires the brain to plan the spacing of the numbers (visuospatial) and translate a complex verbal command into a physical representation (executive function).
A person might have a near-perfect memory but struggle to correctly place the “10 minutes after” hand, signaling that the brain's communication pathways are under stress long before they forget a name or a face.
What Are the Top Cognitive Screening Tests for Dementia Today?
Montreal Cognitive Assessment (MoCA)
The Montreal Cognitive Assessment Exam (MoCA) is widely considered the modern gold standard for early dementia detection and is recommended by current clinical guidelines. It is a 30-point test that takes 10 to 15 minutes to complete and evaluates nine key cognitive domains, including visuospatial and executive function, naming, memory, attention, language, and orientation.
It is highly sensitive (90%-100%) and is particularly effective at catching Mild Cognitive Impairment (MCI) before it progresses to full-blown dementia.
Mini-Mental Status Exam (MMSE) / Folstein Test
Historically, the most common screening tool, the Mini-Mental Status Exam (MMSE), also referred to as the “Folstein test”, is a 30-question test that takes about 5 to 10 minutes. It tests orientation (such as the current date or season), memory (such as recalling three objects), basic math (such as spelling “world” backward or counting backward by sevens), language, and complex cognitive functions, such as drawing a clock.
While still widely used, it is less sensitive than the MoCA and misses many subtle changes in early MCI.
The Mini-Cog
The Mini-Cog screening test for dementia is a brief, simple test that can be completed in just 3 minutes. It consists of a 3-word recall test to evaluate memory and a clock drawing test. Because it requires no special medical knowledge and takes very little time, it is easy to include in regular primary care wellness exams.
Self-Administered Gerocognitive Exam (SAGE)
Unlike tests administered in a clinic, the SAGE dementia screening test is a free, self-administered, pen-and-paper test that can be taken at home. It takes about 15 minutes and consists of 12 questions evaluating memory, reasoning, language, and problem-solving.
It is available in four versions, so patients can take it annually without artificially boosting their scores through memorization.
General Practitioner Assessment of Cognition (GPCOG)
The General Practitioner Assessment of Cognition test (GPCOG) is a screening tool specifically designed for primary care providers. It includes a 4-minute patient assessment, testing time, orientation, clock drawing, reporting a recent event, and word recall.
If the patient's score is indeterminate, an accompanying 2-minute informant interview is conducted with a relative or caregiver to assess the patient's daily functioning, memory of recent conversations, and ability to manage money or medications.
Abbreviated Mental Test Score (AMTS)
The Abbreviated Mental Test Score (AMTS) is a brief 10-item questionnaire that assesses basic orientation and memory. Patients are asked simple questions such as their age, the current time and year, their date of birth, the dates of World War I, and the name of the present monarch. They are also asked to count backward from 20 to 1 and recall an address given to them at the start of the test.
Memory Impairment Screen (MIS)
The Memory Impairment Screening Test for Dementia (MIS) is a brief 4-item test specifically focused on memory impairment. It takes about 4 minutes and involves a delayed-free and cued-recall test, in which the patient must remember words after a 5-minute delay.
The Comprehensive Dementia Screening Chart: A List of Modern Screening Tools for 2026
| Test / Tool Name | Primary Use Case | Key Benefit |
|---|---|---|
| MoCA Clinical |
Early detection (MCI) | Highly sensitive (90%+); catches subtle executive function shifts. |
| Mini-Cog Quick Clinical |
Primary care wellness visits | Fast 3-minute screen evaluating memory and visuospatial health. |
| MMSE / Folstein Traditional |
Middle-to-late stage tracking | Widely recognized; effective for tracking known progression. |
| AMTS Quick Clinical |
Basic orientation | Quick 10-point test often used in acute or emergency settings. |
| MIS Focus: Memory |
Rapid memory check | Short 4-item test specifically for delayed and cued recall. |
| SAGE At-Home |
Starting the conversation | Self-administered; reduces “white coat” anxiety before a doctor visit. |
| AD8 Caregiver-Led |
Informant assessment | 8-question survey capturing functional changes a patient may hide. |
| Short IQCODE Caregiver-Led |
Informant assessment | Brief questionnaire used to flag cognitive concerns alongside patient tests. |
| GPCOG Caregiver + Patient |
Primary Care efficiency | Combines a brief patient test with a caregiver interview. |
| Digital Screens (DCA) Digital/AI |
Precision tracking | Removes human scoring bias; tracks micro-changes over time. |
| FDA-Cleared Blood Tests Bio-Screen |
Rule out Alzheimer's | High-accuracy blood marker to confirm pathology before a specialist referral. |
| RUDAS Specialized |
Multicultural populations | The most “culture-fair” test for non-English speakers. |
| NTG-EDSD Specialized |
Adults with IDD | The gold standard for those with Down Syndrome or other intellectual disabilities. |
Informant-Based Questionnaires for Dementia Involve a Caregiver's Assessment
In addition to testing the patient directly, doctors sometimes use tools that rely on a caregiver or family member's observations.
- AD8 (Ascertain Dementia 8-Item Informant Questionnaire): An 8-question yes/no survey that takes about 3 minutes to complete, assessing changes in the patient's memory, orientation, executive function, and interest in activities over the past few years.
- Short IQCODE: Another brief informant-led dementia assessment used to flag cognitive concerns alongside patient tests.
It is important to note that none of these tests can officially diagnose dementia. They are initial screening tools used to determine if a patient has cognitive impairment, which could be caused by dementia or by treatable conditions such as a urinary tract infection, vitamin deficiency, or sleep apnea.
If a patient scores poorly on any of these screens, a doctor will typically order a full blood panel, neuroimaging, or comprehensive neuropsychological testing to find the true cause.
The Digital Frontier: FDA-Cleared and AI-Powered Screening Test for Dementia
As we move into 2026, the landscape of dementia screening is shifting from pen-and-paper to a digital-first approach. While traditional tests remain foundational, many primary care offices now utilize Digital Cognitive Assessments (DCAs).
These tools, like BrainCheck and Cognivue, offer several advantages: they remove human bias in scoring, track changes more precisely over time, and can often be integrated directly into your medical records.
Beyond standard “thinking” tests, we are also seeing the rise of Digital Biomarkers. Some new platforms use AI to analyze subtle changes in a person’s voice or the way they draw a clock on a tablet – detecting “micro-hesitations” that the human eye might miss.
Furthermore, FDA-cleared blood tests (like the pTau-181) are now becoming a standard “next step” in primary care to help rule out Alzheimer’s pathology before referring a family to a specialist.
Dementia Screening for Everyone: Culturally Fair and Specialized Tools
Standard tests can sometimes be inaccurate for people with different cultural backgrounds or existing disabilities. To ensure every senior gets an accurate look at their brain health, clinicians are increasingly using:
- The RUDAS (Rowland Universal Dementia Assessment Scale): Designed specifically to be “culture-fair,” this test is ideal for those whose first language isn't English or who have had limited formal education.
- The NTG-EDSD: For adults with Down Syndrome or other intellectual disabilities, this specialized tool is the gold standard for tracking the early, unique signs of functional decline.
Conclusion: From Worry to Preparation
The most important takeaway for any caregiver is that cognitive screening is about preparation, not prediction. Whether a loved one’s score is “Normal” (26–30 on the MoCA or above 6 on the AMTS) or falls into the range of impairment, the score is merely a data point to inform your next chapter.
A screening test for dementia is the beginning of a conversation that must include a primary care physician, a full blood panel, and potentially neuroimaging. By choosing to screen for dementia early on, you are not just looking for a diagnosis; you are taking a proactive role in managing your loved one's brain health.
About the Author

Chris is a seasoned healthcare executive and entrepreneur from the Pacific Northwest. He strongly advocates for older adults and the caregivers who serve them. Chris has personal experience caring for his father, who had dementia. Chris is a technology enthusiast and an avid outdoorsman; if he's not in his office, he can usually be found on a golf course or fly-fishing out west somewhere.